
New Scientist Magazine issue 2433 07 February 2004 by Gareth Morgan
crabsallover highlights, key points & comments
IN 1763, a clergyman called Edmund Stone based in the English town of Chipping Norton wrote a letter to the president of the Royal Society, the foremost British scientific body of the time. Stone described his discovery that the powdered bark of willow trees, which commonly grew on riverbanks, helped treat the "agues", or fevers that could afflict those living in damp areas. Stone argued this was proof of the "doctrine of signatures", which stated that nature's remedies gave clues, perhaps by their location, to indicate how they should be used.
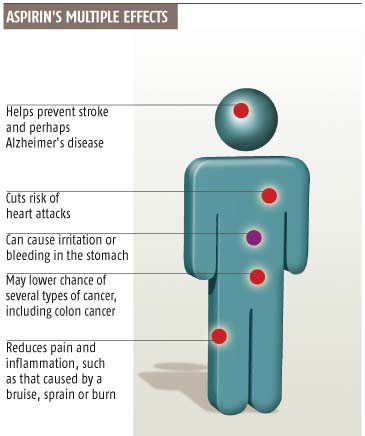
While Stone's line in philosophy failed to make it into mainstream medicine, his finding about willow bark helped drive the development of one of the most widely used drugs in the world today. Willow bark is a rich source of salicylates, the class of compounds to which aspirin (acetylsalicylate) belongs. For more than a century now, people have been taking aspirin to reduce fever and relieve pain, and new benefits from the drug are still emerging. Aspirin's blood-thinning properties make it an excellent long-term treatment to help prevent heart attacks and strokes, and it now appears that the drug could reduce the risk of developing cancer and Alzheimer's disease.
Why should a daily dose of aspirin prevent such a disparate group of diseases? I believe the explanation is that it could have a medical role even greater than that currently appreciated. There is good evidence to suggest that humans' natural diet would once have contained small but significant quantities of salicylates from fruit and vegetables. There is a case for regarding salicylate as a micronutrient, akin to vitamins and antioxidants, that is essential for maintaining good health - perhaps in future we might even call salicylate "vitamin S". If so, this would have important public health implications. Many people might benefit from taking aspirin to increase their chances of staying healthy into old age.
Multi-tasker
So what are aspirin's many effects on the body, and what are their mechanisms? Since aspirin was first patented and marketed in 1899 by German pharmaceutical firm Bayer, other medicines with similar properties have been developed, and they are collectively called non-steroidal anti-inflammatory drugs (NSAIDs). They work by inhibiting the cyclo-oxygenase (COX) class of enzymes, which make prostaglandins, important signalling molecules. There are two kinds of these enzymes, COX-1 and COX-2. The COX-2 enzymes make prostaglandins that are involved in pain and inflammation pathways, giving aspirin its anti-inflammatory effect
It took several more decades before we discovered aspirin's second important effect: reducing cardiovascular disease. At the time the mechanisms behind the formation of the blood clots that could trigger a heart attack or stroke were still unclear. But at the head of each clot, or thrombus, there seemed to be a clump of platelets, tiny cell fragments that are normally suspended in the blood. In the late 1960s, it was discovered that aspirin produced a marked and prolonged reduction in platelet "stickiness". And in 1974, researchers (Peter Elwood et al) at the South Wales MRC Epidemiology Unit in Cardiff showed that this had an appreciable clinical effect. A randomised controlled trial involving over 1000 men who had recently had a heart attack showed that a low dose of aspirin (300 milligrams) reduced deaths by a quarter over two years (British Medical Journal , vol 1, p 436).
Later trials involving many thousands of patients have shown that low-dose aspirin reduces the risk of heart attacks and strokes by at least one-third, and deaths by a quarter. Now, doctors recommend that people who have had a heart attack or a stroke take daily aspirin for the rest of their lives to reduce their chance of a repeat event. Many doctors extend this advice to anyone at risk of a heart attack or stroke - smokers, for example, or people who are obese. Some even advise vulnerable patients to carry a soluble aspirin in case they have sudden severe chest pain.
Why should aspirin stop a heart attack? Platelets clump together because of the action of thromboxane, which is made by COX-1 enzymes, in platelets. Aspirin inhibits COX-1 and so makes platelets less likely to form clots.
COX-1 inhibition is also a key mechanism through which aspirin exerts undesirable effects, most notably stomach irritation and bleeding. Fortunately, serious bleeding and deaths are rare, but patients with a history of stomach problems, such as ulcers, should consult with their doctor before taking aspirin. Low-dose aspirin is reasonably safe, and over 90 per cent of patients take it without experiencing any problems. But the decision to start taking aspirin should always be based on a doctor's judgement that the potential benefits exceed the potential risk.
Aspirin's cardiovascular benefits are now widely documented, and in the past decade, evidence has been accumulating that several years of aspirin use may also reduce the risk of developing certain cancers. We still need the results from large randomised trials to demonstrate the effect, and several are ongoing. But the best evidence so far suggests that the risk of colorectal cancer is reduced by 20 to 30 per cent. There is also suggestive evidence that the drug may reduce the risk of other cancers such as breast (by 20 to 30 per cent), ovarian (20 per cent), gullet (50 per cent) and stomach (50 per cent).
The mechanism of aspirin's anti-cancer effects is not fully understood, but there are several interesting hypotheses. One is that it causes cancer cells to commit suicide (through apoptosis), as this is what happens when cancer cells in the lab are dosed with salicylate. It is believed that impaired apoptosis is one reason why cancers develop, and salicylate is thought to correct this through various effects on COX and non-COX pathways.
If preventing pain, heart disease and cancer weren't enough, it has recently been suggested that aspirin may also reduce the risk of developing Alzheimer's disease, perhaps by more than 10 per cent (British Medical Journal , vol 327, p 128). Although the exact cause of Alzheimer's disease is unclear, one suggestion is that inflammation in the brain is responsible for at least some of the mental deterioration. If so, it may simply be aspirin's anti-inflammatory effects that are responsible, especially as other NSAIDs also appear to be beneficial. The evidence that long-term low-dose aspirin reduces blood levels of C-reactive protein, a marker of inflammation, supports this idea.
Another property of salicylate that could be important is its anti-oxidant effect that counteracts tissue-damaging free radicals produced during metabolic reactions. Free radicals have been implicated in some serious illnesses, such as cancer and Alzheimer's disease, and even the ageing process itself.
So does aspirin confer all these health benefits because salicylate should be a natural component of our diet? Many plant species produce salicylate as a defence mechanism: it induces damaged and diseased cells to commit suicide. Fruits and vegetables that contain high levels of salicylates are therefore more likely to resist damage and disease.
And numerous studies have shown that people who eat more fruit and vegetables have lower levels of heart disease and certain cancers. Is salicylate part of the explanation? Three years ago, a team led by John Paterson at Dumfries and Galloway Royal Infirmary, UK, showed that vegetarian Buddhist monks at a Scottish retreat had higher levels of salicylate in their blood than a non-vegetarian control group. There was wide variation, but the vegetarians' levels overlapped with those of a third group: people taking daily low-dose aspirin (Journal of Clinical Pathology , vol 54, p 553).
Unfortunately many westerners fail to eat enough fruit and veg. A recent survey of over 2000 older men in the Welsh town of Caerphilly showed that only 8 per cent of them eat the recommended five portions of fruit and vegetables per day, and a third consume an average of only one portion a day.
Worse still, the salicylate content of fruit and vegetables is likely to be less than it used to be. Throughout history most people have grown their own fruit and veg or bought them from local market gardens. Because diseases, pests and physical damage would have been common, the salicylate content of the foods would probably have been higher. Now, however, we expect fruit and vegetables in pristine condition. Shoppers often reject produce with bumps or bruises, and modern use of pesticides means plants make little salicylate for self-defence. Another study from the same team in Scotland found that organic vegetable soups contained almost six times as much salicylate as non-organic versions (European Journal of Nutrition , vol 40, p 289).
So thanks to changes in food production and eating habits, we may now be salicylate-deficient. Everyone is constantly exposed to factors that either raise or lower their risk of disease. Salicylate could help to limit the damaging effects of factors that increase disease risk by exerting its anti-inflammatory, antioxidant and apoptotic effects (Pharmacology & Toxicology , vol 93, p 153).
Can salicylate really be considered a vitamin? There is no generally agreed definition of what constitutes a vitamin, but salicylate fulfils at least one of the minimum criteria, in that it is present in the diet, or at least it used to be. And like most vitamins, salicylate can't be synthesised in the body. A third criterion is that trace amounts are essential for the maintenance of life. This is the tricky one: salicylate deficiency itself does not trigger acute symptoms such as the scurvy that accompanies lack of vitamin C, for example. Instead problems seem to develop more slowly, leading to a higher risk of age-related chronic disease. If we consider that lack of salicylate seems to predispose humans to cancer, heart attacks, stroke, Alzheimer's disease, and perhaps other conditions in later life, the compound starts to look increasingly essential - especially given our increasing life expectancy. The late onset of diseases related to salicylate deficiency could be due to accumulating cellular damage and chronic inflammation occurring throughout life.
Counting against aspirin's claim to be a vitamin, on the other hand, is the fact that unlike aspirin, many vitamins are enzyme "cofactors". In other words, they help promote certain biochemical reactions in our cells. Vitamin C, for example, boosts production of collagen, a common structural protein. But at least one vitamin, E, is not a cofactor and is defined as a vitamin purely because it is an antioxidant - a property that salicylates share.
Most vitamins are considered to be essential components of the diet because they cannot be made in the body, but this is not true of vitamins A and D. Vitamin A can be synthesised from a precursor compound in the diet, carotenoid, while vitamin D is made by skin cells exposed to sunlight. So arguably, salicylate is more eligible to be called a vitamin than vitamins A and D, and is at least as eligible as vitamin E.
There are numerous officially classified vitamins - A to H, plus K, M, P, T and V. There is not yet a vitamin S, so salicylate could take that title, with aspirin technically the precursor compound that the body turns into salicylate.
But perhaps we should not worry too much about the name, as the word vitamin is merely a generic term for a disparate group of organic chemicals that have no universally agreed definition. Whatever word we use, there is certainly a case to be made that salicylate is an important micronutrient, a view that seems to be shared by a few other research groups too.
Current dietary patterns suggest that a high proportion of the western population is deficient in salicylates - particularly poorer groups with the worst diets. How can we begin to tackle this public health problem? A range of interventions are theoretically possible, including lifestyle changes, fortification of food and drinking water with synthetic salicylate, changes in food production methods and programmes to encourage more people to take low-dose aspirin. All of these approaches have their drawbacks.
Raising awareness
In terms of practicalities and resources, public health campaigns to boost appropriate uptake of low-dose aspirin show the most promise. Such programmes would be mainly targeted at lower-income individuals, who have higher rates of premature death from cancer and heart attacks. The approach may help to reduce health inequalities between wealthy and poor populations. But at what age should "vitamin S supplementation" be recommended? In an article published last year, I calculated that if people started taking daily low-dose aspirin from the age of 50, they might double their chance of living healthily into their nineties (Medical Hypotheses , vol 60, p 900). Yet you can't take aspirin without clear evidence that benefit exceeds risk, and this highlights the need for more randomised trials of aspirin.
There are other problems with encouraging wider uptake. Aspirin carries no patent, makes very little profit, is inadequately promoted and is seen by some as a rival to other medicines (for example, the cholesterol-lowering drugs statins). So it is vital that national health bodies and the World Health Organization finance extensive research. And while rebranding this chemical as vitamin S would have no legal or regulatory relevance, it might promote a switch in the public perception of aspirin from a drug to a missing component of our diet.
At the very least, the micronutrient theory of salicylate is one more reason for everyone to aim for five daily portions of fruit or vegetables. Does it also suggest we should all switch to organic produce, or that we should choose the most battered and bruised piece of fruit on the supermarket shelf? That is less certain until more research has been carried out. The potential public health benefits are so great that it would be wrong to ignore this important issue.
Bibliography
- The multi-agency Welsh Aspirin Group will hold a meeting about the public health benefits of aspirin in May 2004. For further details contact Gareth Morgan, secretary for the group, at
Gareth.Morgan@nphs.wales.nhs.uk
Gareth Morgan is a public health practitioner at the National Public Health Service for Wales in Swansea. He would like to thank Peter Elwood, Alan Shenkin, Angela Madden and Nick Henderson for their help
No comments:
Post a Comment